
.png?width=1480&height=500&name=tms-therapy-rebates-in-australia_hd%20(1).png)
How does TMS work?
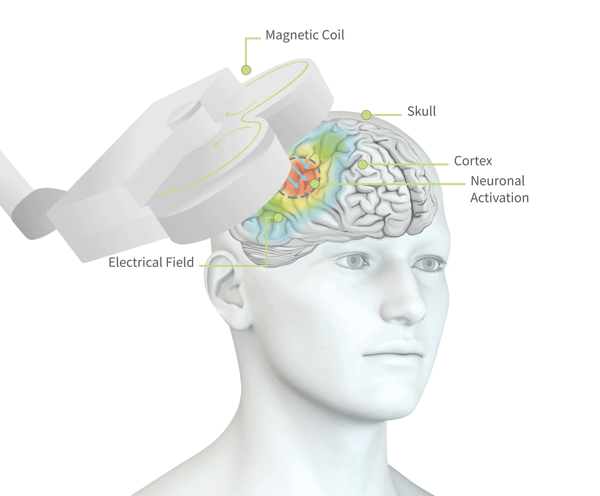
Treatment involves positioning a magnetic coil on your head which delivers a pulse to stimulate specific regions of the brain. The magnetic pulse stimulates nerve cells in a region of your brain involved in mood control and depression.
TMS works particularly well and is highly recommended for those who have not responded to traditional medication for depression or OCD. This type of treatment also avoids the side effects associated with antidepressant medications.
Who can benefit from TMS?

TMS in Depression
TMS is a reliable and efficient treatment for depression. It is highly recommended for individuals who have not seen improvement with medication or other treatment methods.
TMS is also a treatment option for patients seeking to reduce their dosage of antidepressant medication or by those aiming to discontinue medication completely. This course of action should be closely monitored and supervised by a medical professional.
TMS in OCD
TMS is also a potential solution for individuals struggling with Obsessive-Compulsive Disorder. Similar to its use for patients with depression, this treatment is especially beneficial for patients who have not found success with other therapies.
Studies conducted by neurocare clinics in the Netherlands found that the response rate of TMS therapy for patients with OCD, was 55%. A personalized approach to TMS, whereby the patient was also closely monitored to improve their sleep hygiene, is also understood to improve response to treatment.
This technique of combining TMS with other forms of assessment and psychotherapy.
To find out more about TMS and the research behind it, visit our Scientific Publications page.
What to expect when doing TMS therapy

For best results, TMS sessions need to be scheduled daily or at least twice a week. Some patients report antidepressant effects after 5 session, however, it’s important to remember that just as individual causes of depression differ so does the response to treatment. neurocare recommends between 20 to 30 sessions to consolidate the antidepressant effects. You can complete a full course of treatment within one to two months.
At neurocare, TMS sessions are delivered as 60-minute appointments, to also include psychotherapy with a trained mental health professional and treatments are supervised by a psychologist or psychiatrist.
The sessions are conducted in a comfortable treatment chair, where a magnetic coil is placed over your head. The coil generates a pulsating magnetic field, stimulating the target areas within the brain. The magnetic field generates a noticeable ticking sound. While the stimulation is not painful, many patients notice a tingling sensation on their scalp.